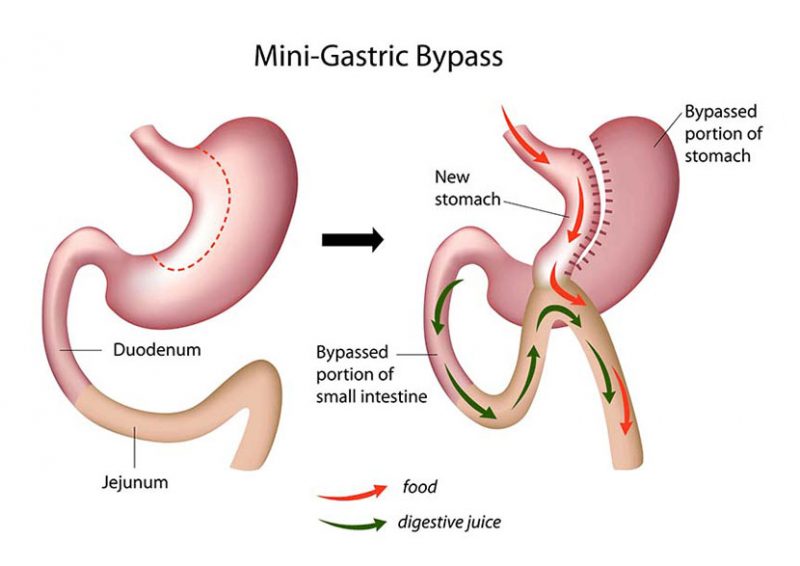
This is a variation on the traditional Roux en Y Gastric Bypass. It offers both restriction and malabsorption but with a single anastomosis between the stomach pouch and small intestine. It offers similar weight loss to that of a traditional RY gastric bypass but with only one anastomosis. The potential side effects include bile reflux that occurs in 5% of patients in which conversion to a formal RY gastric bypass is the only treatment. The recovery and progression through the diet phases is the same.
The theoretical benefit is that there is only one anastomosis that that can leak not two. This procedure is not suitable for patients with acid reflux.
How does it Work
The stomach volume reduction (150-200mL) enables only small amounts of food to be eaten, before satiety (feeling of being full) occurs, stopping the desire to eat further. The bypassed 1.5-2m of small bowel adds a malabsorptive component. This reduces the surface area food can be absorbed from.
Expected Outcomes
Typically patients will lose weight with the the majority losing 50-70% of their excess weight over 2 years. The initial weight loss is more rapid but slows over time. Weight loss does differ between people.
Typical hospitalisation is two nights.
Risks
All operations have risks, general and specific, this list is not comprehensive but includes the most commonly seen ones.
General risks include :
• Bleeding
This is uncommon and is treated at the time of surgery. It typically occurs at the new staple line and only very rarely requires a blood transfusion
• Infection
Uncommon, but occasional occurs at the incision sites and may require a course of oral antibiotics
• Pain
Is typically minimal and simple oral analgesia is required but sometimes stronger pain killers are required.
• Damage to surrounding organs
This is unlikely especially at laparoscopic procedures but damage to the spleen or bowel can occur and this is typically repaired at the time of surgery
• Blood clots (Leg or Lung)
This is rare, and preventative measures such as stockings, and intra-operative calf compression devices are performed routinely. In addition all patients receive blood thinning injections to reduce the risk of clots forming.
Specific Risks
• Staple line leak
This occurs in 0.5- 1% of patients. This allows gastric contents into the abdomen causing infection, and can occur upto 14 days after the operation.
• Stenosis
Excessive scarring occurs at the gastric anastomosis (join) and narrows the lumen preventing easy passage of fluids and food. It occurs in 3% of pateints and requires a gastroscopy with a balloon dilation to enlarge the narrowing.
• Gastric Pouch dilation
Overtime if small meal volumes are not adhered too some patients can stretch the stomach so they can eat larger volumes of food. This results in weight regain, with the only intervention being further surgery.
• Internal hernia
Rarely small bowel becomes caught in the rearranged anatomy and causes a blockage requiring a laparoscopic (keyhole) surgery to remedy.
• Dumping Syndrome
This occurs if too much sugar is ingested at once, causing nausea, dizziness and sweating. Adherence to the dietary plan prevents this occurring.